Total leukocyte count (TLC) refers to the number of white blood cells in 1 μl of blood (or in 1 liter of blood if the result is expressed in SI units). There are two methods for estimation of TLC:
- Manual or microscopic method
- Automated method
A differential leukocyte count should always be performed along with TLC to obtain the absolute cell counts.
The purpose of carrying out TLC is to detect increase or decrease in the total number of white cells in blood, i.e. leukocytosis or leukopenia respectively. TLC is carried out in the investigation of infections, any fever, hematologic disorders, malignancy, and for follow-up of chemotherapy or radiotherapy.
MANUAL METHOD
Principle
A sample of whole blood is mixed with a diluent, which lyses red cells and stains nuclei of white blood cells. White blood cells are counted in a hemocytometer counting chamber under the microscope and the result is expressed as total number of leukocytes per μl of blood or per liter of blood.
Equipment
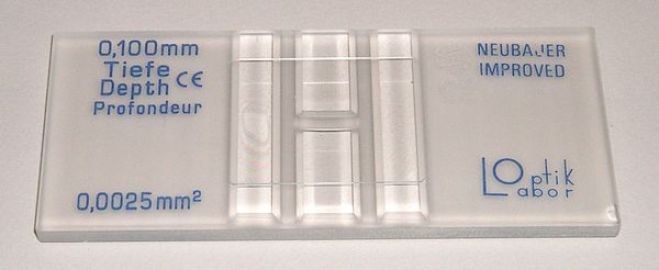
(1) Hemocytometer or counting chamber with coverglass: The recommended hemocytometer is one with improved Neubauer rulings and metalized surface. There are two ruled areas on the surface of the chamber. Each ruled area is 3 mm × 3 mm in size and consists of 9 large squares with each large square measuring 1 mm × 1 mm. When the special thick coverglass is placed over the ruled area, the volume occupied by the diluted blood in each large square is 0.1 ml. In the improved Neubauer chamber, the central large square is divided into 25 squares, each of which is further subdivided into 16 small squares. A group of 16 small squares is separated by closely ruled triple lines. Metalized surface makes background rulings and cells easily visible. The 4 large corner squares are used for counting leukocytes, while the central large square is used for counting platelets and red blood cells. Only special coverglass, which is intended for use with hemocytometer, should be used. It should be thick and optically flat. When the special coverglass is placed on the surface of the chamber, a volumetric chamber with constant depth and volume throughout its entire area is formed. Ordinary coverslips should never be employed since they do not provide constant depth to the underlying chamber due to bowing.
When the special cover glass is placed over the ruled area of the chamber and pressed, Newton’s rings (colored refraction or rainbow colored rings) appear between the two glass surfaces; their formation indicates the correct placement of the cover glass.
(2) Pipette calibrated to deliver 20 μl (0.02 ml, 20 cmm): WBC bulb pipettes, which have a bulb for dilution and mixing (Thoma pipettes) are no longer recommended. This is because blood and diluting fluid cannot be mixed adequately inside the bulb of the pipette. Bulb pipettes are also difficult to calibrate, costly, and charging of counting chamber is difficult. Tips of pipettes often chip easily and unnecessarily small volume of blood needs to be used.
- Graduated pipette, 1 ml.
- Pasteur pipett
- Test tube (75 × 12 mm).
Reagent
WBC diluting fluid (Turk’s fluid) consists of a weak acid solution (which hemolyzes red cells) and gentian violet (which stains leucocyte nuclei deep violet). Diluting fluid also suspends and disperses the cells and facilitates counting. Its composition is as follows:
- Acetic acid, glacial 2 ml
- Gentian violet, 1% aqueous 1 ml
- Distilled water to make 100 ml
Specimen
EDTA anticoagulated venous blood or blood obtained by skin puncture is used. (Heparin should not be used since it causes leukocyte clumping). While collecting capillary blood from the finger, excess squeezing should be avoided so as not to dilute blood with tissue fluid.
Method
(1) Dilution of blood: Take 0.38 ml of diluting fluid in a test tube. To this, add exactly 20 μl of blood and mix. This produces 1:20 dilution. Alternatively, 0.1 ml of blood can be added to 1.9 ml of diluting fluid to get the same dilution.
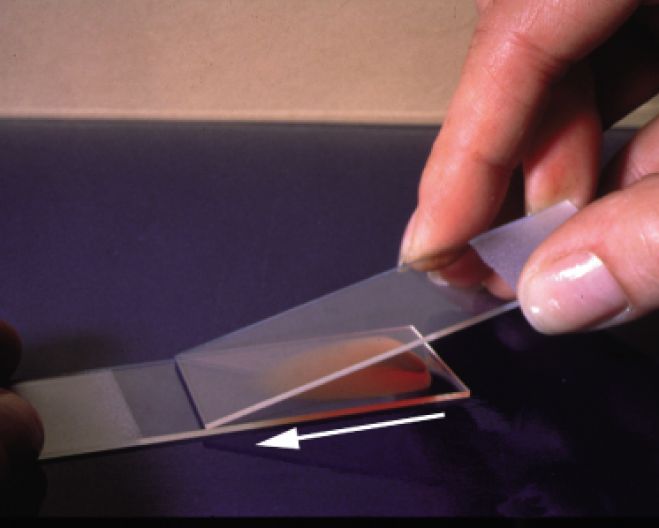
(2) Charging the counting chamber: Place a coverglass over the hemocytometer. Draw some of the diluted blood in a Pasteur pipette. Holding the Pasteur pipette at an angle of 45° and placing its tip between the coverglass and the chamber, fill one of the ruled areas of the hemocytometer with the sample. The sample should cover the entire ruled area, should not contain air bubbles, and should not flow into the side channels. Allow 2 minutes for settling of cells.
(3) Counting the cells: Place the charged hemocytometer on the microscope stage. With the illumination reduced to give sufficient contrast, bring the rulings and the white cells under the focus of the low power objective (× 10). White cells appear as small black dots. Count the number of white cells in four large corner squares. (To reduce the error of distribution, counting of cells in all the nine squares is preferable). To correct for the random distribution of cells lying on the margins of the square, cells which are touching the left-hand lines or upper lines of the square are included in the count, while cells touching the lower and right margins are excluded.
(a) Calculation of TLC:
TLC/μl = Nw x Cd x Cv
NLS
= Nw x 20 x 10
4
= Nw x 50
Where Nw is the number of WBCs counted, Cd is the correction of dilution, Cv is the correction of volume and NLS is the number of large squares counted.
(b) TLC/L = Number of WBCs counted × 50 × 106 (106 is the correction factor to convert count in 1 μl to count in 1 liter). Example: If 200 WBCs are counted in 4 large squares, TLC/μl will be 10,000/μl and TLC/liter will be 10.0 × 109/liter.
If TLC is more than 50,000/ml, then dilution of blood should be increased to 1:40 to increase the accuracy of the result.
If TLC is less than 2,000/ml then lesser dilution should be used.
Expression of TLC: Conventionally, TLC is expressed as cells/μl or cells/cmm or cells/mm3. In SI units, TLC is expressed as cells × 109/liter. Conversion factors for conventional to SI units is 0.001 and SI to conventional units is 1000.
Correction of TLC for nucleated red cells: The diluting fluid does not lyse nucleated red cells or erythroblasts. Therefore, they are counted as leukocytes in hemocytometer. If erythroblasts are markedly increased in the blood sample, overestimation of TLC can occur. To avoid this if erythroblasts are greater than 10 per 100 leukocytes as seen on blood film, TLC should be corrected for nucleated red cells by the following formula:
CTLC = TLC x 100
NRBC + 100
Where CTLC is the Corrected TLC/μl, TLC is the Total Leukocyte Count and NRBC is the Nucleated RBCs per 100 WBCs.
REFERENCE RANGES
- Adults 4000-11,000/μl
- At birth 10,000-26000/μl
- 1 year 6,000-16,000/μl
- 6-12 year 5,000-13,000/μl
- Pregnancy up to 15,000/μl
CRITICAL VALUES
- TLC < 2000/μl or > 50000/μl