Activated Partial Thromboplastin Time (APTT)
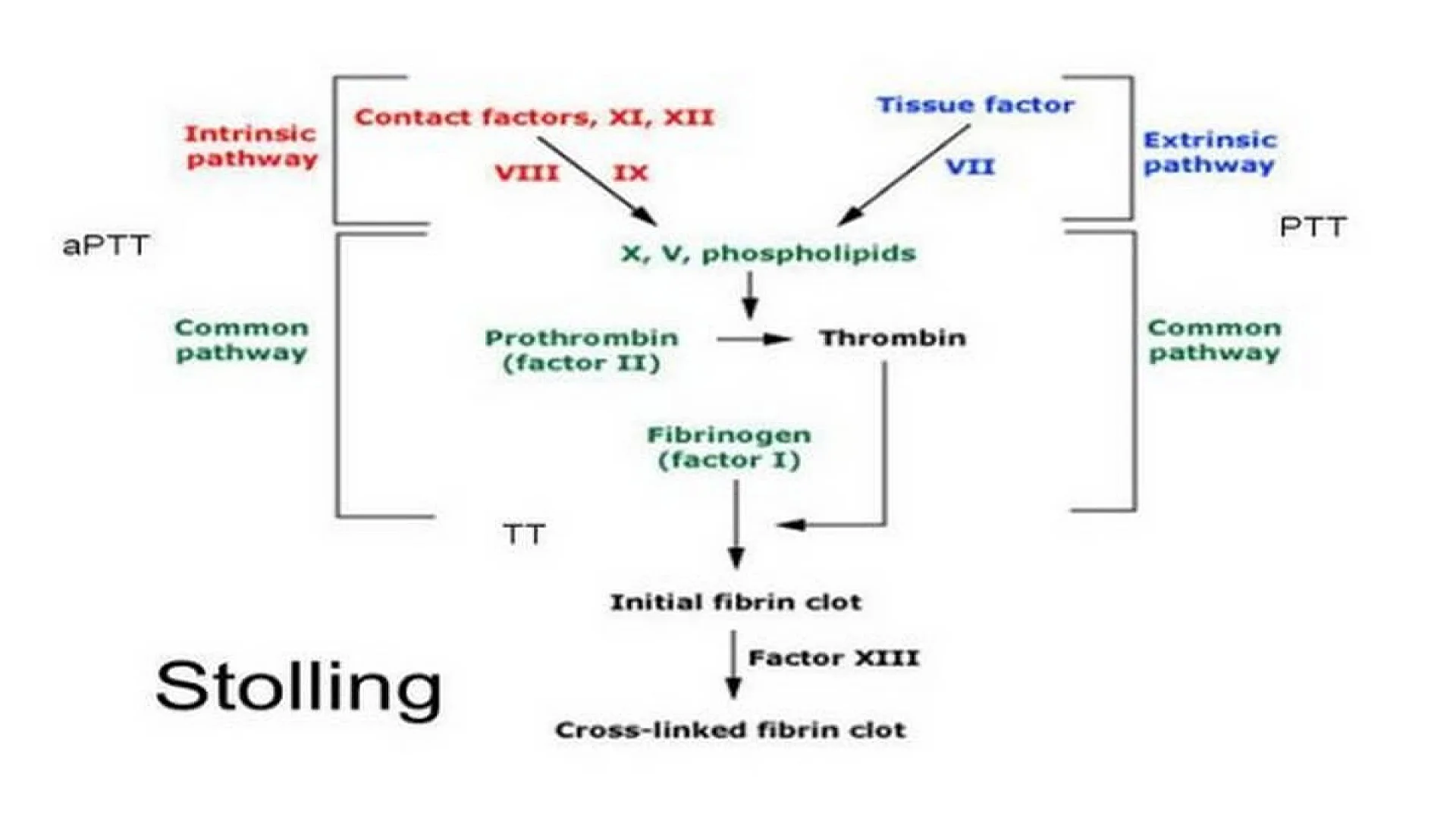
APTT is a measure of coagulation factors in intrinsic pathway (F XII, F XI, high molecular weight kininogen, prekallikrein, F IX, and F VIII) and common pathway (F X, F V, prothrombin, and fibrinogen).
APTT is a measure of coagulation factors in intrinsic pathway (F XII, F XI, high molecular weight kininogen, prekallikrein, F IX, and F VIII) and common pathway (F X, F V, prothrombin, and fibrinogen).
Principle
Plasma is incubated with an activator (which initiates intrinsic pathway of coagulation by contact activation). Phospholipid (also called as partial thromboplastin) and calcium are then added and clotting time is measured.
Equipment
This is same as for Prothrombin Time test.
Reagents
- Kaolin 5 gm/liter: This is a contact activator.
- Phospholipid: Various APTT reagents are available commercially, which contain phospholipids.
- Calcium chloride 0.025 mol/liter.
Specimen
This is same as for Prothrombin Time test.
Method
(1) Mix equal volumes of phospholipid reagent and calcium chloride solution in a glass test tube and keep in a waterbath at 37°C.
(2) Deliver 0.1 ml of plasma in another test tube and add 0.1 ml of kaolin solution. Incubate at 37°C in the waterbath for 10 minutes.
(3) After exactly 10 minutes, add 0.2 ml of phospholipidcalcium chloride mixture, start the stopwatch, and note the clotting time.
Normal Range
30-40 seconds.
Causes of prolongation of APTT
- Hemophilia A or B.
- Deficiencies of other coagulation factors in intrinsic and common pathways.
- Presence of coagulation inhibitors
- Heparin therapy
- Disseminated intravascular coagulation
- Liver disease
Uses of APTT
- Screening for hereditary disorders of coagulation: Since deficiencies of F VIII (hemophilia A) and F IX (hemophilia B) are relatively common, APTT is the most important screening test for inherited coagulation disorders. APTT detects deficiencies of all coagulation factors except F VII and F XIII. PT is also performed along with APTT. Prolongation of both PT and APTT is indicative of deficiency of coagulation factors in common pathway. Normal PT with prolongation of APTT is indicative of intrinsic pathway deficiency (particularly of F VIII or IX).
- To monitor heparin therapy: Heparin potentiates the action of natural anticoagulant antithrombin III which is an inhibitor of thrombin and activated factors IX, X, and XI. Full dose heparin therapy needs monitoring by APTT to maintain the dose in the therapeutic range (1.5 to 2.5 times the upper reference limit of APTT).
- Screening for circulating inhibitors of coagulation: APTT is prolonged in the presence of specific inhibitors (which are directed against specific coagulation factors) and non-specific inhibitors (which interfere with certain coagulation reactions).
Mixing experiment for detection of inhibitors: Mixing studies are used to distinguish between factor deficiencies and factor inhibitors (specific coagulation factor inhibitor or non-specific inhibitor such as lupus anticoagulant). If APTT is prolonged, patient’s plasma is mixed with an equal volume of normal plasma (called as a 50:50 mix) and APTT is repeated. In coagulation factor deficiency, prolongation of APTT gets corrected by more than 50% of the difference between the clotting times of control and test plasma. In the presence of lupus anticoagulant, there is no such correction. With lupus anticoagulant, APTT remains prolonged after mixing and for 2 hours following incubation. With F VIII inhibitor (which is time- and temperature-dependent), prolonged APTT gets immediately corrected after mixing, but becomes prolonged after incubation.
The information on this page is peer reviewed by a qualified editorial review board member. Learn more about us and our editorial process.
Last reviewed on .
Article history
- Latest version
Cite this page:
- Comment
- Posted by Dayyal Dungrela