New Cholesterol Guidelines Say Start Earlier to Prevent Heart Disease
A major update to cholesterol management urges earlier screening, personalized risk scoring, and more aggressive prevention strategies to curb heart disease decades before it begins.
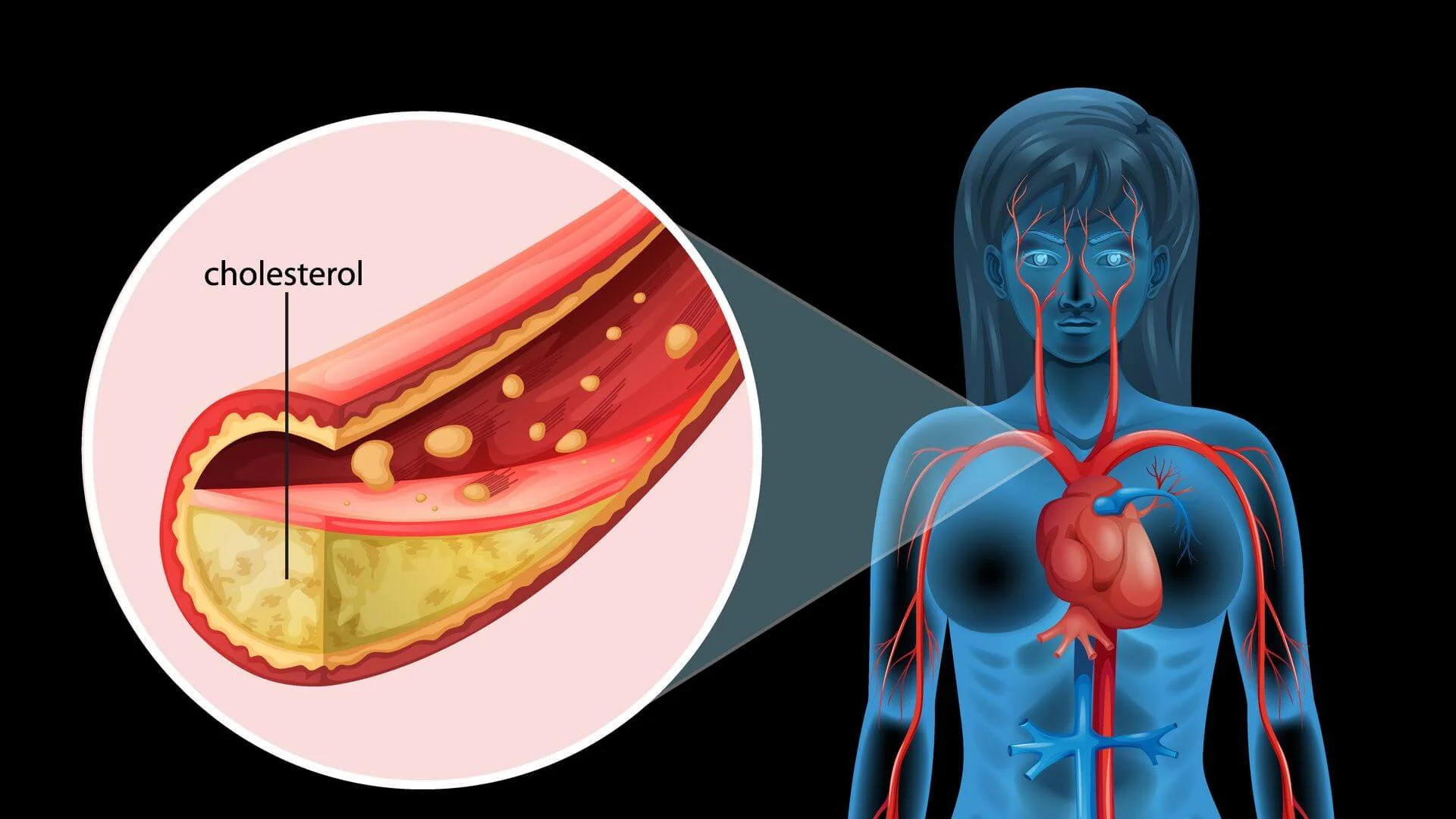
Heart disease rarely begins with a sudden crisis. Instead, it develops silently over years, even decades, as fatty particles circulate in the blood and gradually settle into artery walls. By the time symptoms appear, much of the damage is already done.
A new set of clinical guidelines aims to change that timeline.
Published by leading cardiovascular organizations, the 2026 recommendations represent a shift in how scientists and clinicians think about cholesterol. Rather than reacting to disease later in life, the focus now moves toward identifying risk earlier and acting sooner, long before arteries begin to narrow.
At its core, the update reflects a growing realization: the cumulative exposure to harmful cholesterol matters just as much as the levels measured at a single moment.
A Shift Toward Earlier Prevention
The most striking message in the new guideline is simple but transformative. Prevention should begin earlier, sometimes decades earlier than before.
Researchers highlight that cholesterol-related damage can start in adolescence. Even moderately elevated levels of low-density lipoprotein cholesterol, often called LDL or “bad” cholesterol, can gradually increase the lifetime risk of cardiovascular disease.
The guideline recommends earlier screening in both children and adults, particularly for those with a family history of heart disease. It also encourages clinicians to consider treatment sooner in certain individuals, even if their short-term risk appears low.
This approach reflects a long-term view of cardiovascular health. Instead of focusing only on the risk of a heart attack in the next ten years, the new strategy accounts for the total burden of cholesterol exposure over a lifetime.
Rethinking How Risk Is Calculated
A major update in the guideline involves how cardiovascular risk is estimated.
Traditionally, clinicians have relied on older models to calculate a person’s likelihood of developing heart disease. The new recommendations replace these with a more modern system known as the PREVENT risk equations.
This model allows for a more nuanced understanding of risk across a broader age range, particularly in adults between 30 and 79 years old. It categorizes individuals into low, borderline, intermediate, or high risk based on their probability of developing cardiovascular disease.
But the guideline does not stop at simple calculations.
It introduces a three-step framework:
- First, calculate baseline risk
- Second, personalize that risk using additional factors
- Third, refine the estimate using imaging or further testing if needed
This layered approach acknowledges that no single number can fully capture an individual’s health profile.
New Biomarkers Offer Deeper Insight
Beyond standard cholesterol tests, the guideline places new emphasis on additional biomarkers that can reveal hidden risk.
One of the most important is lipoprotein(a), or Lp(a), a genetically influenced particle linked to cardiovascular disease. The guideline recommends that all adults have Lp(a) measured at least once in their lifetime.
Elevated levels of Lp(a) are associated with significantly higher risk, even when traditional cholesterol levels appear normal. Identifying this early can help guide more aggressive prevention strategies.
Another marker gaining attention is apolipoprotein B, or ApoB. This protein reflects the number of atherogenic particles in the blood, offering a more precise measure of risk in some individuals, especially those with diabetes or elevated triglycerides.
Together, these markers provide a more detailed picture of cardiovascular health, moving beyond the traditional focus on LDL alone.
Imaging the Invisible
In some cases, the guideline recommends going a step further by directly assessing the arteries themselves.
Coronary artery calcium (CAC) scoring, obtained through imaging scans, can detect early signs of plaque buildup. Even in people without symptoms, the presence of calcium in the arteries indicates underlying atherosclerosis.
The new recommendations expand the use of CAC scoring to refine risk estimates, particularly in individuals where treatment decisions are uncertain.
For example:
- A CAC score of zero may support delaying medication in some low-risk individuals
- Higher scores suggest a need for more aggressive treatment
This approach allows clinicians to tailor decisions more precisely, avoiding unnecessary treatment in some cases while identifying hidden risk in others.
Lower Targets, More Aggressive Treatment
Another key update involves treatment goals.
The guideline reintroduces specific cholesterol targets alongside percentage reductions. This dual approach provides clearer benchmarks for both clinicians and patients.
For individuals at higher risk, the recommended LDL levels are now lower than in previous guidelines. In some cases, targets fall below 70 mg/dL, and for very high-risk individuals, even below 55 mg/dL.
Achieving these levels often requires a combination of therapies.
While statins remain the cornerstone of treatment, the guideline highlights additional options, including:
- Ezetimibe
- PCSK9 inhibitors
- Newer agents such as bempedoic acid and inclisiran
These therapies can be added when statins alone are not sufficient to reach target levels.
Lifestyle Still Forms the Foundation
Despite advances in medications and diagnostics, the guideline reinforces a familiar message.
Lifestyle remains the foundation of cholesterol management.
Healthy eating patterns, regular physical activity, weight management, adequate sleep, and avoiding smoking all play a central role in reducing cardiovascular risk.
However, the guideline also acknowledges the limits of lifestyle changes alone. For many individuals, especially those with genetic predispositions, medication may be necessary even with optimal habits.
Interestingly, the recommendations advise against relying on dietary supplements for lowering cholesterol, citing inconsistent evidence and limited benefit.
Special Populations and Personalized Care
The updated guideline expands its scope to address a wide range of populations, reflecting the complexity of cardiovascular risk.
It includes tailored recommendations for:
- People with diabetes
- Individuals with chronic kidney disease
- Those living with HIV
- Cancer survivors
- Pregnant individuals
Each group has unique risk factors and treatment considerations, underscoring the importance of personalized care.
The guideline also introduces reproductive risk factors, such as early menopause or pregnancy complications, as part of cardiovascular risk assessment. These factors have often been overlooked in traditional models.
Why This Matters
Cardiovascular disease remains the leading cause of death worldwide, yet much of it is preventable.
The new guideline suggests that earlier and more precise intervention could significantly reduce this burden.
By identifying risk sooner, refining how it is measured, and treating it more aggressively when needed, the approach aims to alter the trajectory of disease long before symptoms appear.
In practical terms, this could mean fewer heart attacks, fewer strokes, and healthier aging for millions of people.
What Still Remains Uncertain
Despite its comprehensive scope, the guideline acknowledges several gaps in current knowledge.
There is still uncertainty around:
- The long-term effects of newer therapies
- Optimal strategies for integrating genetic testing
- The evolving impact of emerging risk factors such as vaping and cannabis use
Ongoing research will be essential to refine these recommendations further.
The guideline itself is designed to evolve, incorporating new evidence as it becomes available.
A New Direction for Cardiovascular Prevention
Taken together, the 2026 cholesterol guideline marks a significant evolution in cardiovascular care.
It shifts the focus from reactive treatment to proactive prevention. It embraces more precise tools for assessing risk. And it encourages earlier, more individualized intervention.
Most importantly, it reframes cholesterol not as a short-term concern, but as a lifelong factor shaping cardiovascular health.
The message is clear. The earlier the action begins, the greater the opportunity to prevent disease before it takes hold.
The guidelines have been published in the Journal of the American College of Cardiology.
This content has been reviewed by subject-matter experts to ensure scientific accuracy. Learn more about us and our editorial process.
Last reviewed on .
Article history
- Latest version
Reference(s)
- Blumenthal, Roger S. Blumenthal., et al. “2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia.” Journal of the American College of Cardiology, 13 March 2026, doi: 10.1016/j.jacc.2025.11.016. <https://doi.org/10.1016/j.jacc.2025.11.016>.
Cite this page:
- Posted by David Anderson