Modified Bloom–Richardson Grading System: Histological Basis, Scoring Criteria, and Clinical Significance
The Modified Bloom–Richardson grading system, widely used in breast cancer pathology, evaluates how tumor cells differ from normal breast tissue. By analyzing gland formation, nuclear features, and mitotic activity, this system predicts tumor behavior.
The Modified Bloom–Richardson grading system, also referred to as the Nottingham grading system, is a histopathological method used for grading invasive breast carcinoma. It provides an objective assessment of tumor differentiation and serves as a critical prognostic indicator in breast cancer evaluation. The system is based on the microscopic appearance of the tumor and reflects the biological behavior, aggressiveness, and potential outcome of the disease. By combining structural, nuclear, and mitotic features, this grading method helps pathologists determine how closely tumor cells resemble normal breast tissue.
Historical Background
The original Bloom–Richardson system was introduced in 1957 by Bloom and Richardson, who proposed a histological grading method for breast carcinoma based on three morphological parameters: tubule formation, nuclear pleomorphism, and mitotic activity. Their goal was to establish a correlation between microscopic appearance and clinical behavior of the tumor.
In 1991, Elston and Ellis at Nottingham City Hospital modified this original system to provide clearer scoring criteria, reduce observer variability, and improve prognostic accuracy. Their refined approach became known as the Modified Bloom–Richardson (MBR) system or the Nottingham grading system, which is now the universally accepted standard for grading invasive ductal carcinoma of the breast.
Principle of the System
The fundamental principle of the Modified Bloom–Richardson system is that the degree of tumor differentiation correlates with its biological aggressiveness. Well-differentiated tumors resemble normal breast tissue and tend to have a better prognosis, while poorly differentiated tumors show marked structural and cytological atypia with more aggressive clinical behavior. The system evaluates three histological parameters: tubule formation, nuclear pleomorphism, and mitotic count. Each parameter is scored on a scale from 1 to 3 according to the degree of abnormality, and the sum of these scores determines the final grade.
Histological Parameters Assessed
1. Tubule (Glandular) Formation
This criterion assesses how much of the tumor maintains normal glandular architecture. The presence of tubules indicates differentiation toward normal glandular structures.
- Score 1: More than 75% of the tumor shows tubule formation.
- Score 2: Between 10% and 75% of the tumor shows tubule formation.
- Score 3: Less than 10% of the tumor shows tubule formation.
A higher score signifies a loss of glandular differentiation, which corresponds to a more aggressive tumor.
2. Nuclear Pleomorphism
Nuclear pleomorphism evaluates variation in the size, shape, and chromatin pattern of tumor cell nuclei. It reflects the degree of cellular atypia and genetic instability within the tumor.
- Score 1: Nuclei are small, uniform, and resemble normal epithelial cell nuclei.
- Score 2: Nuclei show moderate variation in size and chromatin distribution.
- Score 3: Nuclei are large, irregular, hyperchromatic, and markedly pleomorphic.
The assessment of nuclear pleomorphism requires careful comparison with normal ductal epithelial cells in the surrounding tissue.
3. Mitotic Count
The mitotic count measures the number of actively dividing cells and reflects the proliferative activity of the tumor. It is determined by counting the number of mitotic figures in ten consecutive high-power fields (HPFs) in the most cellular areas of the tumor.
The cut-off points for scoring vary depending on the microscope field diameter, as field area affects the number of cells seen. Generally, the following pattern applies:
- Score 1: Low mitotic activity.
- Score 2: Moderate mitotic activity.
- Score 3: High mitotic activity.
A standardized field diameter must always be reported to ensure reproducibility of results across laboratories.
Calculation of Final Grade
The three individual scores (1–3) for each histological parameter are added to yield a total score ranging from 3 to 9. The sum corresponds to the final histological grade as follows:
| Total Score | Histological Grade | Tumor Differentiation |
|---|---|---|
| 3 – 5 | Grade I | Well differentiated (low grade) |
| 6 – 7 | Grade II | Moderately differentiated (intermediate grade) |
| 8 – 9 | Grade III | Poorly differentiated (high grade) |
This grading helps classify the tumor into prognostic categories and guides therapeutic decision-making.
Microscopic Features of Each Grade
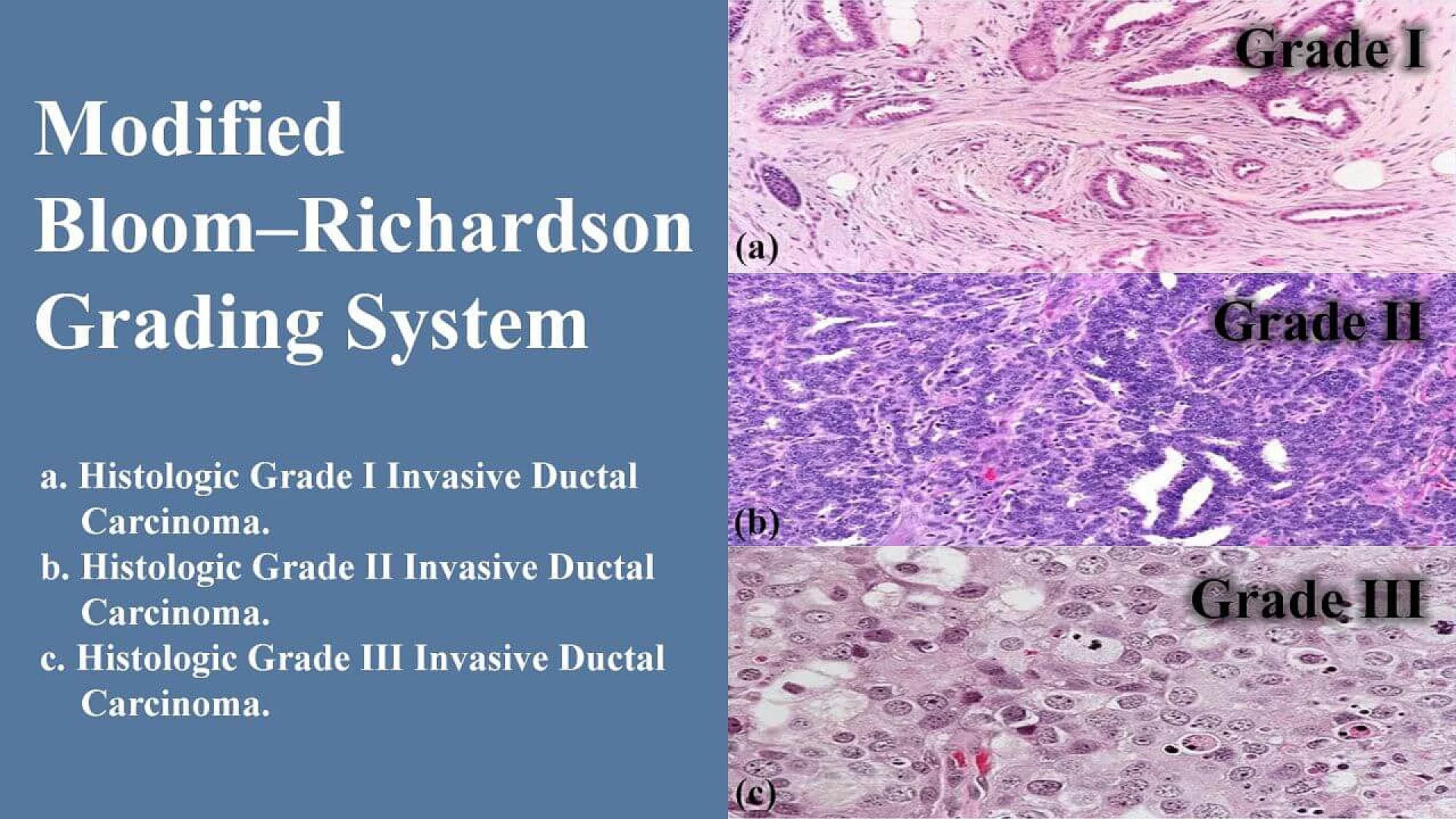
Grade I (Well Differentiated)
These tumors closely resemble normal breast tissue. Tubule formation is extensive, nuclear atypia is mild, and mitotic activity is low. Patients with grade I tumors generally have a favorable prognosis and respond well to standard therapies.
Grade II (Moderately Differentiated)
These tumors show partial loss of glandular architecture and moderate nuclear variation. Mitotic figures are more frequent than in grade I. The prognosis is intermediate and clinical behavior may vary.
Grade III (Poorly Differentiated)
These tumors exhibit minimal tubule formation, marked nuclear pleomorphism, and high mitotic activity. They are biologically aggressive, more likely to metastasize, and associated with poorer survival outcomes.
Clinical Importance and Prognostic Significance
The Modified Bloom–Richardson grade is a powerful independent prognostic factor in breast carcinoma. It provides vital information regarding tumor aggressiveness, likelihood of recurrence, and overall survival. Histological grade correlates with other prognostic indicators such as lymph node status, tumor size, and hormonal receptor profile (ER, PR, HER2). In clinical practice, the histological grade, when combined with receptor status and proliferative markers such as Ki-67, helps determine treatment strategies, including the need for chemotherapy or hormonal therapy.
Advantages of the Modified Bloom–Richardson System
- High reproducibility: The defined criteria minimize observer variation compared to the original Bloom–Richardson method.
- Strong prognostic correlation: The final grade closely correlates with clinical outcome and disease-free survival.
- Simplicity and cost-effectiveness: The assessment requires only routine hematoxylin and eosin-stained sections, making it applicable even in resource-limited settings.
- Universal acceptance: It is recommended by major cancer research and pathology organizations as the standard method for grading invasive breast carcinoma.
Limitations
Although reliable, the Modified Bloom–Richardson system has some limitations. The mitotic count can vary due to differences in fixation time, section thickness, and microscope field size, leading to potential scoring variability. Nuclear pleomorphism remains somewhat subjective, especially in borderline cases. The grading system is most accurate for invasive ductal carcinoma and may not fully represent the behavior of special histological subtypes such as medullary, mucinous, or tubular carcinoma, which can show distinct biological patterns despite their grade.
Role in Modern Breast Cancer Evaluation
With the advancement of molecular pathology, newer prognostic models incorporate molecular markers and gene expression profiles. However, histological grading using the Modified Bloom–Richardson system remains fundamental in diagnostic pathology. It complements molecular testing by providing morphological evidence of tumor differentiation and proliferation. Even in the era of precision medicine, the histological grade continues to play a central role in breast cancer classification and management.
Practical Considerations for Pathologists
To ensure accuracy and consistency:
- Always evaluate well-preserved areas of the tumor.
- Avoid necrotic or hemorrhagic regions when counting mitoses.
- Use a standardized field area and record it in the report.
- Compare nuclear features with adjacent normal ductal cells.
- Record individual parameter scores along with the final grade for transparency.
A well-documented grading report contributes to better patient management and facilitates interdisciplinary communication among oncologists, surgeons, and radiologists.
Conclusion
The Modified Bloom–Richardson grading system is a cornerstone of breast carcinoma assessment and remains indispensable in routine histopathology. It provides an objective, reproducible, and clinically meaningful evaluation of tumor differentiation and proliferation. Despite the growing emphasis on molecular diagnostics, this grading method continues to serve as an essential tool for prognosis and therapeutic planning. The combined assessment of morphological features within this system reflects the biological behavior of the tumor and assists clinicians in making evidence-based treatment decisions.
The information on this page is peer reviewed by a qualified editorial review board member. Learn more about us and our editorial process.
Last reviewed on .
Article history
- Latest version
Reference(s)
- Johns Hopkins Pathology. “Staging & Grade - Breast Pathology.” Johns Hopkins Pathology <https://pathology.jhu.edu/breast/staging-grade/>.
- Meyer, John S., et al. “Breast carcinoma malignancy grading by Bloom–Richardson system vs proliferation index: reproducibility of grade and advantages of proliferation index.” Modern Pathology, vol. 18, no. 8, doi: 10.1038/modpathol.3800388. <https://www.sciencedirect.com/science/article/pii/S0893395222045781>.
Cite this page:
- Posted by Dayyal Dungrela